What Happened to the Pandemic of the Unvaccinated?

The COVID-19 vaccines promised to 1) stop the transmission of COVID-19, 2) reduce the viral load in COVID cases, 3) provide long-term protection, and 4) reduce severe symptoms associated with COVID-19.
Three of the four promised benefits of the vaccines were proven to be wrong. Is it that far of a stretch to suspect that the final promise is highly questionable too? If you receive three falsehoods with no apologies, why would you expect the forth promise to be true?
To elucidate the forth promise, we’ve witnessed the use of the most unprovable metric to demonstrate effectiveness.
When someone is vaccinated and then gets COVID anyway, you can test for that. When someone is vaccinated and then has a high viral load anyway, you can test for that. When the efficacy of vaccine-derived immunity wanes, you can test for that. But when someone is vaccinated, gets COVID anyway, and then says, “At least the vaccine kept me out of the hospital,” how could you possibly know that without testing it?
When someone says, “I got COVID after I was vaccinated, but at least it kept me from getting hospitalized or dying.” You can’t go back in time, remove the shot from their arm, and then see the natural response of their immune system versus the perceived vaccine-induced immune response. Their belief is inherently theoretical.
They could simply (and far more likely) be one of the approximately 9 out of 10 people who didn’t have severe outcomes from COVID prior to the vaccines being in existence. Yet, credit is illogically given to a novel drug that failed to stop them from getting the disease in the first place. The credit goes to the drug because of a preconceived bias, not because it’s actually provable beyond a reasonable doubt.
Simply ask yourself some logical questions:
Why is it that these vaccines don’t stop disease transmission, don’t consistently reduce viral load, don’t provide promised levels of protection very long, yet they seemingly appear to reduce hospitalizations? And why do they reduce hospitalizations by enormous numbers predominantly in the U.S. and not in other notable countries with comprehensive data sets like Israel and the U.K.? Why is the U.S. the outlier in hospitalizations?
These are very important questions for understanding whether, at least, one of the four vaccine promises are actually true and how our systems of analysis and reporting currently work. Let’s deconstruct the data and deliver some helpful clarity.
1) The causes of hospitalizations are not properly adjudicated and have not been since the onset of COVID, leading to rampant confounding factors in data collection and imprecise reporting. The proper reporting of the underlying reason for hospitalizations and death have been, in no more fitting of a description, a dumpster fire.
It doesn’t help that the data is sullied by the fact that the U.S. population is so extraordinarily unhealthy. To put it into a sobering description, the U.S. is the most chronically diseased nation in documented human history. Approximately 245 million U.S. citizens are overweight or obese, 130 million citizens have diabetes or prediabetes, nearly 60% of the population have some degree of heart disease, 70 million citizens have digestive diseases, upwards of 50 million citizens have autoimmune diseases, and this is just for starters. With approximately 45 percent of the U.S. population being clinincally obese and trending up, we’re set to cross half of the population being clinically obese within the next few years. There isn’t a word to describe how troubling this is.
There are a whole host of reasons why this matters, from our decaying quality of life to our exploding economic burden. But why this matters in the context of COVID was highlighted in an analysis of over 800 U.S. hospitals and over 540,000 COVID-19 patients published by the CDC. The report found that obesity is the NUMBER ONE risk factor for death from COVID-19. The second leading risk factor for death is anxiety and fear-related disorders (pointing to our tragic state of mental health), while the third leading risk factor is diabetes and related complications.
Our gumbo of deadly, predominantly lifestyle-related diseases makes accurate reporting for causes of death and hospitalizations a nightmare. According to the CDC, nearly 95% of people who died with a reported COVID-19 infection had an average of FOUR preexisting chronic diseases and/or comorbidities. With a supermajority of reported deaths being from a population of remarkably sick people with other deadly issues besides COVID, it will inherently spark a clumsy debate on how serious COVID really is.
Part of the issue in gaining clarity from the data is the polarity that’s taken place between people who believe COVID isn’t a big issue and people who believe that COVID is the only issue.
It should never be an issue of whether COVID is real or not, it’s an issue of accurately studying and determining whether COVID is the actual reason for hospitalization and poor outcomes or not. This has been a challenge since the very beginning. Now, even Dr. Anthony Fauci (03:18) and other health officials are coming forward to call for clarity on someone being hospitalized for another issue but happening to have COVID versus someone who is hospitalized because of COVID. Keeping in mind that nearly 9 out of 10 people who’ve contracted COVID had moderate to no symptoms at all, it’s a huge population majority of people who will be carrying COVID at any given time and potentially seeking medical attention for an unrelated issue. A vaccine does not change the fact that accurate reporting has been unreliable, at best.
2) Since the beginning of the vaccine campaign, under the false premise that vaccines stop the transmission of COVID-19 (which was stated by everyone from the head of the CDC (00:34) to the President of the U.S. (09:18) and then parroted incessantly by the media until it became accepted as truth), the enforcement has been to test the unvaccinated and not the vaccinated, as it is the unvaccinated who are the real threat.
A common requirement has been to, “Show your vaccine card or proof of a negative test,” in order to work, go to school, attend events, and much more. For instance, this was the requirement for individuals to attend the Super Bowl in Los Angeles this year (a mega event happening while the city was under a “state of emergency,” mind you). Nevermind the fact that vaccinated individuals can carry and spread COVID just as easily, it is the unvaccinated that need to test. And at the stadium they even had “free testing on site in front.”
Healthcare and social systems suddenly pushed for lots of testing of unvaccinated citizens (the ones who needed to provide proof that they’re not a threat) while simultaneously allowing vaccinated individuals to refrain from testing. In fact, nearly a year ago, the CDC thought so little of the growing number of breakthrough infections in vaccinated individuals that they openly shared they would no longer monitor COVID cases in the majority of vaccinated people. They stated, "(The) CDC transitioned from monitoring all reported COVID-19 vaccine breakthrough infections to investigating only those among patients who are hospitalized or die.” This is simply not appropriate from a logical data perspective, because nearly 9 out of 10 COVID cases are mild or asymptomatic in vaccinated individuals (nearly the same severity as the general population prior to the vaccines being in existence nonetheless) but, since they declared they would no longer monitor these breakthrough infections, we have no idea how much the vaccinated population contributed to the continued progression of the pandemic.
To add injury to insult, they also noted in the report that, “the number of reported COVID-19 vaccine breakthrough cases is likely a substantial undercount of all SARS-CoV-2 infections among fully vaccinated persons." Yet, they're outwardly saying we're not going to look into it any further.
They also noted that vaccinated persons likely “might not seek testing.” Which furthers my point of the lacking urgency for vaccinated persons to be tested equally.
Why would they not seek testing? Well, another ingrained discouragement for vaccinated individuals to be tested lies in the statement that, “vaccine side effects are normal.” After vaccination, people are programmed to expect that symptoms of sickness are simply their immune system responding to the treatment.
The reality is, they very well could get COVID after they are vaccinated. This is why the accepted moniker of being “fully vaccinated” doesn’t kick in until 14-days after the second dose (in the case of the novel mRNA vaccines). In the meantime and in between time, if you get sick it’s likely the vaccine and not covid, so no need to worry (more psychological disuation). Remember, you’re already “partially protected.”
And for months at the beginning of the vaccine campaign, people wrongly believed that the vaccines stopped transmission. So, even after they were “fully vaccinated,” if they got sick, it must be the flu, a cold, allergies, or anything else. It obviously isn’t COVID because they’re protected from that.
Unfortunately, this false belief will inherently take place with our healthcare professionals as well. The inconsistencies in testing and reporting are staggering (as you’ll see more of in #4 below).
But the achilles heel of this reporting system once it reaches the hospital setting is the unreliability of vaccine status being a black or white “Vaccinated” or “Unvaccinated/Unknown”. Many data sets are not denoting a clear vaccination status.
In fact, the way notes are written in a non-systematic way across various hospital settings creates another troubling confounding factor. In a recent study conducted by researchers at the FDA, they worked with other researchers (including operatives at IBM) to create an algorithm that clarifies records from hospital notes to better discern vaccine status and adverse events. The analysis uncovered a 16.8% increase in the identification of vaccine administrations compared to using structured data alone. This means that there should have been 16.8% more hospitalizations that were counted as vaccinated and 16.8% less hospitalizations counted as unvaccinated or unknown. This is more than a 33% shift from the numbers that were reported!
In many ways, our current systems have created uneven, unreliable testing and outcome data. And that leads us to the most important discernment in this data analysis.
3) All of the data showing that these vaccines (that wane quickly, don’t stop transmission, and don’t reduce viral load) are somehow fiercely reducing hospitalizations and deaths are based on OBSERVATIONAL data. Observational data can denote a correlation, but it does NOT confirm causation. By its very nature, observational data is subject to an enormous amount of biases and confounding factors.
This scientific tenet seems to have been completely abandoned and observational data has suddenly become an unquestionable fact. Observational data is meant to complement (affirm or implore the action of) controlled clinical trials.
A randomized, placebo-controlled trial is considered to be the gold-standard for drug testing. It’s where you have a specific treatment (in this case a vaccine) and monitor for specific results (in this case a reduction in hospitalizations and severe outcomes).
To get EUA approval for these novel vaccines (let’s use Pfizer and Moderna’s mRNA technology in this instance), the drug companies submitted their actual randomized, placebo-controlled clinical trial data. So, the obvious question would be, how did the vaccines actually perform under stricter conditions that eliminate biases? Did the vaccines significantly reduce the risk of hospitalizations and death? Absolutely not. And you’re about to find out exactly how it was misconstrued.
This leads us into the difference between socially accepted sound bites from health officials and the media (even if they’re not intentionally trying to be deceptive) and a real analysis of the clinical trial data. When the mRNA vaccine campaigns began, the promise of a “95% effectiveness” was being touted without context.
The “95% effectiveness” and “94% effectiveness” of the Pfizer and Moderna vaccines, respectively, were the perceived relative risk reduction in the clinical trials. The relative risk reduction can function as a comparative clinical figure that compares one group to another, for example. But the relative risk reduction does not denote the reduced risk for an individual in the real world. The true effectiveness of a treatment for you, as an individual in the real world, would be denoted by the absolute risk reduction. The absolute risk reduction is the most useful and appropriate way of presenting research results, especially for the general public who have no experience in discerning the difference in clinical trial outcomes. And as detailed in this analysis of the mRNA vaccine trials, “The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that affects the interpretation of vaccine efficacy.”
So what was the absolute risk reduction of the mRNA vaccines found to be in the clinical trials? In other words, what would be the effectiveness of the vaccines to protect you, as an individual, in the real world? Well, the absolute risk reduction of the Pfizer vaccine wasn’t 95%, it wasn’t 50%, it wasn’t 10%, it wasn’t even 1%. The absolute risk reduction offered to you by the Pfizer vaccine was an unimpressive 0.7% risk reduction. And the absolute risk reduction of the Moderna vaccine wasn’t much better at a 1.1% risk reduction for you in the real world. This was far different from the lofty 94% effectiveness that was being promoted far and wide.
But that’s just the thing. It’s not that the 94% effectiveness was a lie. It was the relative risk reduction found in their clinical trial data. But presenting that number to the public and policymakers without context is the problem. It’s misleading to omit what someone’s personal risk reduction would be if they were to roll up their sleeve and be injected with this newly formulated technology. If news anchors and health officials were to look into the cameras and say, “You can look forward to less than a 1% risk reduction with this new Pfizer vaccine and a 1.1% risk reduction with the Moderna vaccine,” it would obviously not inspire people to run out and get vaccinated. And, at minimum, it would likely inspire a lot more healthy skepticism and inquiry.
Now, this leads us to the most important aspect of the clinical trial data in regard to accurate data collection in the real world. When the vaccines were promised to deliver 95% effectiveness, it was a 95% effectiveness to do what, exactly?
It might be assumed that the 95% effectiveness meant effectiveness in reducing your risk of catching COVID, preventing the transmission to others, or reducing your risk of death or hospitalization. But none of that would be true. In actuality, not a single one of those were primary endpoints found in the trials. The 95% effectiveness demonstrated in the trials was for reducing your risk of “mild to moderate” symptoms. The vaccine clinical trials did NOT show a significant reduction in risk of contracting COVID and they did NOT show a significant reduction in being hospitalized or dying from COVID either. The trials only showed a slight 0.7% absolute effectiveness (in the case of Pfizer) in preventing you from having a mild to moderate COVID infection. That is all. Nothing more.
And the trial data was affirmed in a real world setting if anyone cared to look. It’s a cleaner data set as it’s in a country that didn’t have “intermingling” of different vaccines. The Israeli mass vaccination campaign utilized the Pfizer–BioNTech vaccine. Although the design and methodology are different from the randomized trial design, the researchers reported a relative risk reduction of 94% (nearly the same as in the clinical trial), but with an absolute risk reduction of 0.46%, which was comparable to the less than 1% risk reduction noted in the clinical trial, but not even providing individuals with half a percent of protection in the real world.
The bottomline: The original clinical trial data did not satisfy the primary claims made by health officials and regulatory agencies. The efficacy of the mRNA vaccines were based on prevention of mild to moderate COVID-19 infections. The controlled clinical trial data did not conclude that the vaccines substantially prevented hospitalizations, severe disease, or death, nor did the data conclude prevention of infection and transmission potential.
This is precisely why it wasn't a surprise that the vaccines didn’t stop the spread of COVID-19 as promised. There was nothing to indicate that they would! The confusion arises when clinical trial data is ignored and observational data, with all of its confounding factors and biases, becomes infallible fact. Even the early OBSERVATIONAL data from the Israeli vaccine campaign noted reductions in infection rates and severe outcomes in vaccinated individuals versus unvaccinated individuals. But, suddenly, and repeatedly, the cases and severe outcomes in their vaccinated citizens became dominant, as did the rise in severe side effects like myocarditis in teen boys and young men. One report published in Science noted that the incidence of myocarditis in young men after vaccination was 5 to 25 times higher than the background rate without being vaccinated.

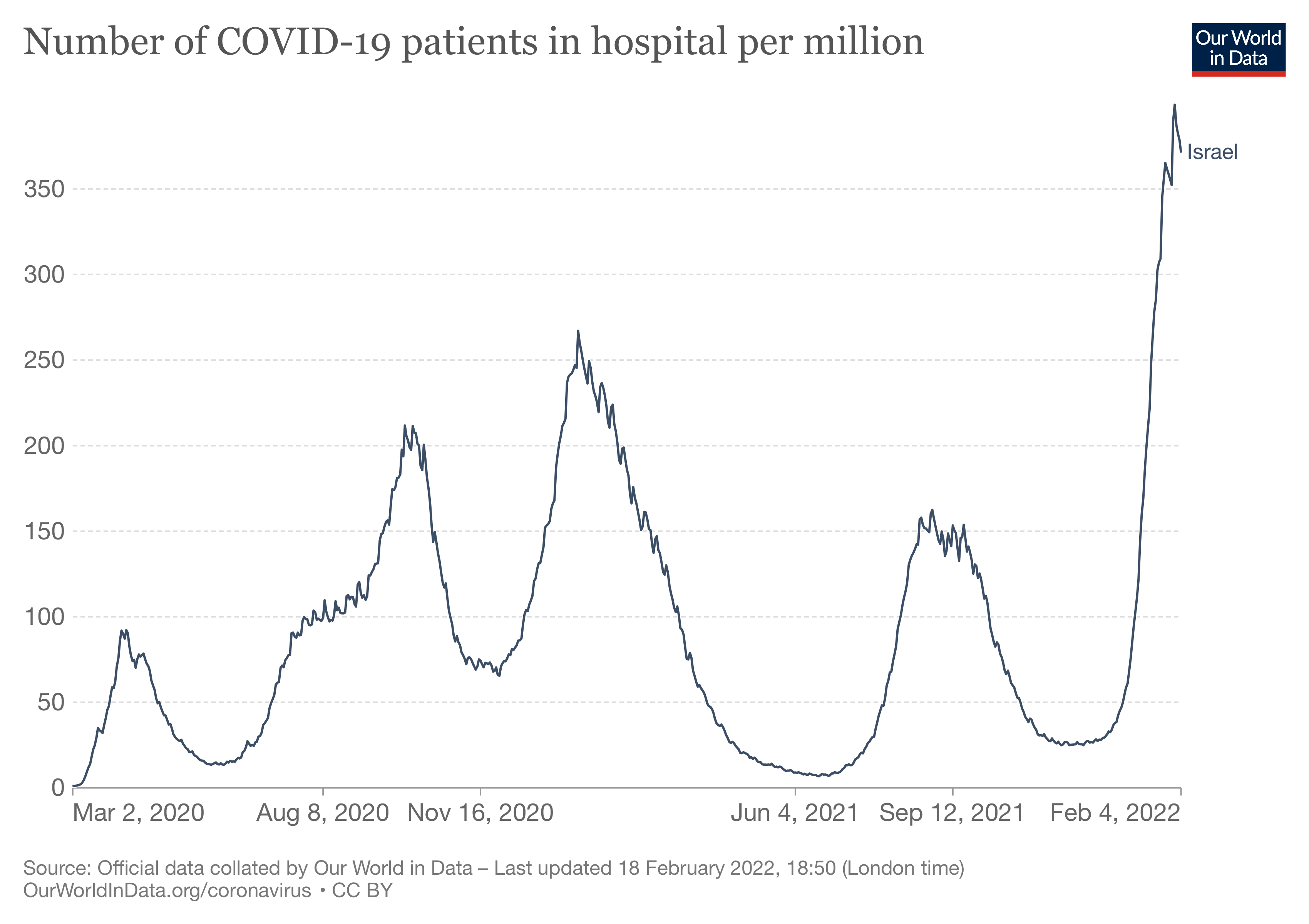
Despite Israel having one of the most vaccinated populations on Earth, as their vaccine efficacy plummeted, and cases, hospitalizations, and deaths in vaccinated individuals continued to hit record numbers, it’s explained away as “it’s waning protection (you just need to be triple or quadruple vaccinated),” or “it’s because so many people are vaccinated,”or “it’s because the vaccines are not effective against variants…” All of these things are theories based on OBSERVATIONAL data that can be distorted in countless ways. Even this article from CNBC, that notes the effectiveness of the Pfizer vaccine plummeting from 95% effectiveness to just 39% effectiveness in Israel all the way back in July 2021, ignores the smoking gun of concern and pivots to more unsubstantiated theories. In essence, the article says, “Hey everyone, the vaccine effectiveness tanked to just 39%, but it’s still 80 - 90% effective at preventing you from getting seriously sick.” Forget the fact that prior to the vaccines being in existence, 80 - 90% of COVID cases were mild or asymptomatic anyways. They’re using doublespeak. It’s framing things for an uneducated, trusting public to maintain a narrative.
If observational data is sufficient and headline worthy, why has the public not heard about the report published by Public Health England (page 12) on the alarming death rate of hospitalized patients who were vaccinated? The death rate among fully vaccinated patients (26 out of 4,087) was 0.636%. The deaths among unvaccinated patients (34 out of 35,521) was 0.0957%. The death rate among fully vaccinated patients was 6.6 times higher than unvaccinated patients in this study. This should be shocking. Not only from the perspective of the outcome, but from the perspective that observational data can be so varied depending on where you choose to look.
Again, the clinical trial data did not show that COVID vaccines substantially reduce the risk of severe symptoms, hospitalizations, and death. It’s an incredible manipulation on the part of health officials and regulatory agencies to make the public think otherwise. Once the misleading data reaches healthcare workers and the public at large who are starving for good news, the false idea spreads like an unstoppable wildfire. It no longer matters if the idea is true or not, every logical argument against it is burned down in its path. All that’s seen are objects that fuel the fire while manipulated humans search for things to affirm the false belief. This is when tremendously low quality, unreliable observational data steps in to pour gasoline on the fire and scorch the earth with the “pandemic of the unvaccinated.”
4) Observational data is easily corrupted or blatantly misinterpreted. One of the reports that was cited countless times, purporting that 99% of the people being hospitalized with COVID-19 were unvaccinated, was published by The Associated Press. But if you’re just caught up in a spicy headline, you’ll miss the most important two sentences in the entire article:
“The Associated Press analyzed figures provided by the Centers for Disease Control and Prevention. The CDC, itself, has not estimated what percentage of hospitalizations and deaths are in fully vaccinated people, citing limitations in the data.”
Limitations in the data was an understatement. They had no business putting together their hodge-podge interpretation of the data that the CDC, itself, cited multiple limitations on, and then publishing it as if it were gospel.
The incomplete and easily misinterpreted data was very similar to this report on the effectiveness of vaccines to reduce hospitalizations published by the CDC in September 2021. The report teed things off with the applause-worthy stats of vaccine effectiveness against COVID-19 hospitalization. Moderna’s effectiveness was a glowing 93%, Pfizer showed a robust 88% effectiveness, and Johnson & Johnson’s effectiveness was a respectable 71%. But there was something incredibly deceptive about the data. The people who had immunocompromising conditions (that could include anything from diabetes, to heart disease, to cancer, to obesity, to dementia, to liver disease, to mental health conditions, and a myriad of other issues—basically any of the conditions that the vast majority of the U.S. population has), even if they were vaccinated, were eliminated from the vaccinated count.
Not only did they eliminate more than half of the people hospitalized with COVID from the data count, they highlighted the fact that they did it like it was a good thing. Basically, “We don’t want these sick people defiling our clean vaccinated data.” And to make matters worse, in order to maintain a narrative-consistent “vaccinated or unvaccinated” classification, they even excluded people hospitalized who were vaccinated, but just not to their liking.
In their words, “Patients with immunocompromising conditions were excluded… Patients were excluded if they received a COVID-19 vaccine other than Moderna, Pfizer-BioNTech, or Janssen; received one or more vaccine doses but did not meet criteria for full vaccination; or received doses of two different COVID-19 vaccine products.”
Why does this matter? It paints a very deceptive picture of who’s actually being hospitalized with COVID. People with immunocompromised conditions represent the MAJORITY of U.S. citizens. There is no ethical reason to omit them from the data if this were truly about informing the public and policymakers about who’s at the greatest risk of being hospitalized. In fact, one of the dominant narratives of this vaccination campaign was to provide protection for those who “need protection the most.” What if that protection for people with preexisting conditions wasn’t working as promised? All you need is a sleight of hand in collection of observational data to make the unfavorable numbers disappear.
Now, the next logical questions would be:
How many of the immunocompromised people did the vaccines fail in this analysis? Are the vaccination statuses of the immunocompromised people who were hospitalized with COVID noted in the report? Nope, of course not.
But we can easily discern that a significant percentage of them were vaccinated. In a report published in the Lancet by researchers at the FDA and several other prestigious institutions, they stated that because immunocompromised individuals are highly vulnerable to COVID-19, they were “prioritized for early immunization” and are “plausibly more likely to be offered and seek vaccination.”
So, they excluded the very people who were promoted to need protection the most, plus eliminated a huge chunk of people from the study who were vaccinated in various ways, and what is left is a misleading vaccinated versus unvaccinated hospitalization depiction that shows vaccines working stunningly well. The truth is, of the people analyzed in this report, about 42% of the people hospitalized with COVID were unvaccinated, 6% were (healthy) vaccinated, and a damning 51% were excluded! There were 1,786 human beings who were excluded—936 for having an underlying health condition (who, statistically speaking, had a significant probability of being vaccinated) and 566 people who were vaccinated but did not meet their “eligibility criteria.”
The inclusion of the people who were excluded from the trial would dramatically shift the ratio of people who were hospitalized with COVID that the public is hearing about. But the problem is deeper than that. It’s the very cookie-cutter vaccinated versus unvaccinated status that they literally can just make up what constitutes as vaccinated or not. Under the criteria in this published CDC analysis, you can have two shots in your arm, be after your 14-day marinating period, catch COVID, end up hospitalized, and still not be counted as a vaccinated hospitalization due to a crafty technicality. When the stakes are so high, and everything is so contentious, there is simply no way that misdirective data like this is appropriate.
Let’s examine one more recent report published by the CDC on hospitalizations in California and New York. This data, again, does not denote a causal relationship in any way to vaccines and hospital admissions as it appears to on the surface. And in the true form of observational data that’s reaching with a preconceived narrative, this data is so sporadic and unreliable that it borders on being incoherent garbage.
For instance, the report states that during the week of May 30, 2021, COVID-19 case rates were 19.9-fold lower in vaccinated individuals without a previous infection versus unvaccinated individuals without a previous infection in California and 18.4-fold lower in New York. Then, shockingly, by the week of October 3, 2021, the difference between vaccinated versus unvaccinated case rates without a previous infection plummeted from 19.9-fold lower to only 6.2-fold lower in California and from 18.4-fold lower to 4.5-fold lower in New York. The presumed protection against hospitalizations dropped more than 3 times lower in California and more than 4 times lower in New York! This was not part of the promise. But with observational data, you can kick in with the excuses, “it’s a different variant,” “the protection diminishes over time,” etc. The clinical trial data never showed that the vaccines protect against other variants and they never showed that the perceived protection stays high over time. These are not “surprise” outcomes. These are observations of the expected idiocy from believing something will do what it was never supposed to do.
Now, here’s where data like this gets even more incoherent and unreliable. During the week of May 30, 2021, COVID-19 case rates were 7.2-fold lower in unvaccinated individuals with a prior COVID-19 diagnosis versus unvaccinated individuals without a previous diagnosis in California and 9.9-fold lower in New York. Then, just 4 months later, the perceived benefit of having a previous infection (i.e. natural immunity) takes a gigantic leap. The case rate among unvaccinated persons with a prior COVID-19 infection is now 29-fold lower than unvaccinated persons without a previous infection in California and 14.7-fold lower in New York. The perceived protection from a previous infection jumped up 4 TIMES higher in the state of California in just 4 months. In New York, it went up notably as well, but nothing compared to the jump in California. Now, herein lies one of the smoking guns of absurdity in relying on the credibility of observational data like this to inform public health policy and public education…
The perceived protection from having a prior COVID-19 infection jumped from 7.2-fold to 29-fold in four months in the state of California. And the perceived protection from having a prior infection jumped from 9.9-fold to 14.7-fold in the state of New York over that same time period. How in the world is natural immunity 29-fold better in the state of California while it’s only 14.7-fold better in the state of New York?
The natural immunity found in California is nearly twice as effective as what you’d find over the 4 and a half-hour flight distance in New York. How? Why? What are the confounding factors causing this? It can range from a myriad of environmental issues, to administration issues, to reporting issues, to… on and on and on. This type of observational data has no context. And using it to inform the public and guide healthcare policy is unethical.
Humanity has invested countless years into refining the scientific method and perceiving valid, factual data versus conjecture. And this type of data published by the CDC that still proposes a magical benefit from COVID vaccines whose perceived effectiveness (admittedly) plummets dramatically, is a disrespect to the high-quality science and data analysis we now have the capacity to do.
Now, here’s the thing about this analysis that can easily be overlooked amidst all of the cheerleading of the vaccines whose perceived benefit fails to deliver what it was publicly promised. This study is also (reluctantly) highlighting the fact that natural immunity rose above the effectiveness of vaccine-derived immunity.
By the week of October 3, 2021 in California, compared to unvaccinated people without a previous COVID infection, case rates in among vaccinated people who didn’t have a previous infection were 6.2-fold lower, while the case rates among unvaccinated people who had natural immunity from a previous infection were 29.0-fold lower! This is a striking demonstration of superiority of natural immunity over vaccine-derived immunity. Yet, numerous studies, discussions, and even people’s experience within the topic of natural immunity have been censored, and even banned, from social media platforms like Facebook and Instagram. These acts of censorship overtly suppress the credibility of the innate human immune system while propping up the validity of novel drugs that don’t remotely perform as advertised (and happen to make tens of billions of dollars for pharmaceutical companies with a long criminal history of fraud, bribery, and death).
It’s not just a coincidence that these same pharmaceutical companies provide billions of dollars each year to various government agencies, drug reviewers, and individual government officials.
It’s not just a coincidence that these same pharmaceutical companies spend billions of dollars each year “educating” and cajoling doctors into using their products (that largely do not fix health issues and often become a revolving cash cow for the drug company).
It’s not just a coincidence that these same pharmaceutical companies provide billions of dollars in funding to major media outlets who significantly influence public perception.
The CDC’s own study demonstrates an aspect of natural immunity that’s superior to vaccine-derived immunity, yet the media, health officials, and health policy makers have framed natural immunity as if it’s a floating possibility. When well over 99% of the infectious diseases that humanity has ever faced have been overcome by natural immunity. The existence of natural immunity has never been in question. What deserved to be in question is the artificially derived immunity from newly invented biologics that, as the data indicates, wear out faster than fake jewelry. All the while, it’s been a gold rush for drug companies who are capitalizing on the collective ignorance and fear of our population.
The tens of billions made from the first series of vaccines weren’t enough. When they failed the first time, the framing just shifted to, “You just need another!” That’s what a booster is. It’s a cute name for another vaccine. Now, how do we keep the cash cow mooing? We get seasonal COVID vaccines in rotation… added to the list of flu shots once the flu remembers that it doesn’t have to pretend to have disappeared anymore.
Is it possible that the dramatic jump in natural immunity (jumping up nearly 5 times higher in California, for example) and the dramatic decline in vaccine-derived immunity (dropping more than 3 times lower over the course of just 4 months) was actually just the way it always was? Could the time passing just help to flesh out how things really are? Could the early observational numbers denoting vaccine benefit over the unvaccinated have included biased data that includes locations and time spans when data was not being uniformly and accurately recorded?
The changes in numbers that show increasingly disfavorable results for the vaccines are so startling in just a short period of time that you can’t help but wonder how things appeared to be so effective to begin with. Again, you can explain it away with talk of variants (why release it then when multiple variants were already documented and circulating in the population and you have NO IDEA how it will perform against those variants? I guess you’ll just wait and see when the human lab animals give you the low-quality observational data that you can manipulate?). You can explain it away with cute terms like “waning protection” and “breakthrough infections.” But what those terms mean is that the vaccine FAILED and that failure has become the norm. When millions of vaccinated people contract the virus anyway, it’s no longer a “breakthrough infection,” it’s an infection.
Unless you accurately test and report everyone in a controlled environment to extract a clean data set (like the outbreak cluster in Massachusetts that was published by the CDC as well), then the observational data will be a hodgepodge of questionable data at best, or corrupted, unethical data at its worst.
The results from the COVID-19 outbreak cluster in Massachusetts, conducted by the Massachusetts Department of Public Health et al., were far different from the prevailing narrative. After analyzing the data from the large public gathering and outbreak, 469 COVID cases were identified, 74% of the cases were in FULLY VACCINATED individuals, and 80% of the individuals hospitalized were fully vaccinated. Where are the stories about that from the talking heads on network news? Why didn’t health officials or, at least, the head of the CDC (the very entity that published the report), come out and say, “It looks like we may have gotten it wrong about the vaccines stopping the spread of COVID. Again, this observational study denotes that 80% of the people hospitalized were fully vaccinated. Which is more in alignment with the report published just a couple weeks later from Israel finding that nearly 60% of gravely ill patients are fully vaccinated versus the wildly illogical, unproven catchphrase that “99% of the people hospitalized are unvaccinated.”
Yes, it’s a shocking difference from the prevailing narrative, but we must remember that we cannot rely on any observational data to be the infallible law of the land, regardless of how much it can refute or affirm our beliefs because…
5) The confounding factors and glaring holes in the vaccine campaign are bigger than you may realize. If we rely on observational data, alone, we’ll never really know where any perceived benefit or harm actually comes from. There are often too many confounding factors at play. Even strange, unexpected things can befuddle outcomes in the data. In fact, any positive benefit or harm derived from a vaccine could’ve literally been from what the person believed about the vaccine.
Researchers at Beth Israel Deaconess Medical Center at Harvard University detailed how more than two-thirds of the rampant number of adverse events reported from COVID vaccines were all in the people’s heads. Researchers proclaimed that it was a negative placebo effect (aka nocebo effect) that was to blame. Now, we could take the time to deconstruct how much conflicting data is in the study, but this pithy, viral headlined article has a wonderful sentence that highlights things for you.
The report on the clinical trial states, “Shockingly, nearly a quarter of the people—some who received the placebo shot—experienced side effects like a sore arm, also attributable to the placebo effect.” So, according to the researchers, having a sore arm from getting a shot in the arm is relegated to a placebo effect? This is a perfect example of how published data from very prestigious entities can venture right into the ridiculous.
In the trial data, itself, it describes the placebo group (receiving saline injections) as having significantly less adverse events than the people receiving the drugs, but the placebo group also experienced notable side effects such as arm pain and headaches. Interestingly, some of the most well-established side effects from a saline injection include… you guessed it… arm pain and headaches.
Let’s just glance over the fact that 61.4% of the people who received the actual COVID-19 vaccine had an adverse event after their second shot. Information like that doesn’t beat the catchy headline that two-thirds of people experiencing vaccine side effects are manufacturing the side effects with their mind.
What’s even more interesting is that just a month earlier, researchers from the very same institution at Beth Israel Deaconess Medical Center, published data on the positive placebo benefits that can come from the belief in the drugs themselves. They dig in on how the belief in the treatment, and/or the act of getting a treatment, alters our biochemistry in ways that have a therapeutic effect. This mind-body connection is the basis for the fields of psychoneuroendocrinology and psychoneuroimmunology. Your thoughts instantly create correlating chemistry in your body that can either enhance or suppress healthy function, including the function of your immune system.
Negative mental states based on fear and anxiety can have a devastating impact on the body, as noted in the study published by the CDC that included over 540,000 COVID-19 patients. The researchers found that anxiety and fear-related disorders are the 2nd leading risk factor for death from COVID-19. The cascade of stress-related hormones being produced in the body can damage cells, increase systemic inflammation, and tear our system down from the inside out if fear and anxiety are not managed healthfully. What happens when people are inundated with fear and worry over catching COVID for weeks or even months on end? It dramatically suppresses immune function. So, have the media and fear-mongering politicians been complicit in the poor health outcomes seen by our citizens during this time? You already know the answer to that. Fear can kill. But, getting back to this study from Beth Israel Deaconess Medical Center, positive belief can heal.
The placebo effect (the belief that a drug or fake drug is having a beneficial impact) is actually so strong that it constantly causes problems in clinical trial data. As one report on the befuddlement that placebos cause in clinical trials states, “...the placebo effect is quite troubling to the pharmaceutical industry, as their drugs have to be better than placebo (literally, better than nothing) to be approved for use—and they often struggle to meet that mark.” The placebo effect consistently produces significant results in clinical trials. But the effect appears to get even stronger when the treatment is injected into the body.
Several studies indicate that the placebo benefits of injections are even stronger than that of pills. Like the study published in the Journal of Neurology on oral versus injected placebo treatments to reduce the severity of migraines. Yes, injections were found to outperform oral treatments in the study, but the most astonishing aspect (that can be easily overlooked) is that placebo injections reduced the severity or eliminated migraines in participants over 32 percent of the time! The belief that it would help them made it help them. And research cited in the journal Frontiers in Psychiatry sought to explain this phenomenon by stating, “The greater effect of placebo devices (like injections from needles) compared with placebo pills may be due to the additional physical contact or the tactile component of the intervention, which is minimally present with the use of pharmaceutical pills.
Has the placebo effect been a factor in the harms, benefits, and even lack of effectiveness of the COVID-19 vaccines seen in the observational data? Based on the decades of research we have on the placebo effect, it very likely has. But to what extent, we’ll never know. Because the nature of relying on observational data makes it impossible. The placebo effect could’ve had a major impact or a tiny impact. Either way, it’s impossible to prove it or disprove it.
We could’ve extracted more viable data on the placebo outcomes as things played out if we had the actual randomized, placebo-controlled trials to refer to. But, during the trial, and after their vaccines were given emergency use authorization, Pfizer and Moderna broke the protocol and notified the control group that they were not really given the vaccine.
They were then offered the opportunity to be vaccinated, and the vast majority of the control group were then given the vaccine… under the guise that it was the righteous thing to do so that they’re not left out of its miraculous protection. This decision automatically left essentially no viable randomized clinical trial data to measure long-term safety and effectiveness of their vaccines.
Dr. Steven Goodman, a clinical trials specialist at Stanford University, says losing those control groups makes it more difficult to answer some important questions about COVID-19 vaccines. "We don't know how long protection lasts," he says. "We don't know efficacy against variants—for which we definitely need a good control arm—and we also don't know if there are any differences in any of these parameters by age or race or infirmity."
His assessment of the high-quality data we’d lose came months before we found out that the promised protection doesn’t last very long, before we found out that there’s terrible efficacy against variants, and before we saw how these vaccines don’t actually reduce your risk of getting the infection and transmitting it to others.
The report goes on to say, “Clinical trials that include a placebo group are the surest and most definitive ways to gather information about vaccine effectiveness.” But by cutting the cord on the placebo-controlled trials out of the kindness of their hearts, what did the vaccine companies really do? They left our potential of tracking vaccine harms and benefits up to observational studies that are easily manipulated by all of the points we’ve covered here. Could it have been an intentional “out” on the part of the vaccine companies to prove safety and efficacy? We’ll have to leave that up to speculative, biased observational data as well.
And one more thing to take note of if we’re going to allow observational data to be the law of the land in this pervasive vaccine campaign. The best observational data that we have has revealed a plethora of serious adverse events from vaccines on a scale that we have never seen before. From myocarditis in young people, to abnormalities in reproductive health in women, the data that we have available is quite alarming. An analysis of the Vaccine Adverse Events Reporting System (VAERS) co-run by the CDC and FDA found an over 1,100% increase in adverse events from COVID-19 vaccines in 2021 versus the number of adverse events from all vaccines combined over the past ten years.
Obviously, one could say that the observational data in VAERS does not prove causality. And, if that’s the case, I want them to remember that same scientific tenet the next time they hear a study presuming vaccine effectiveness from observational data as well.
Our citizens deserve a comprehensive education. Our citizens deserve to have a fair risk-benefit analysis. Our citizens deserve to have informed consent to make decisions that they feel good about.
I have learned a lot from your work, keep it up good sir!
Thank you sir for what you are doing. I share your work with anyone who will read it!